
The Estrogen Withdrawal Effect: A Precise Guide to Protecting Your Hair During Hormonal Transitions

You are standing in the shower. The drain is clogged - again. You pull a fistful of hair from the wall tile where you pressed it so you wouldn't have to watch it disappear. You tell yourself it is normal. You tell yourself it will stop.
But weeks pass. Then months. The ponytail gets thinner. The part gets wider. And nobody gave you a roadmap for this.
Here is what is actually happening.
The Biology Behind the Drop
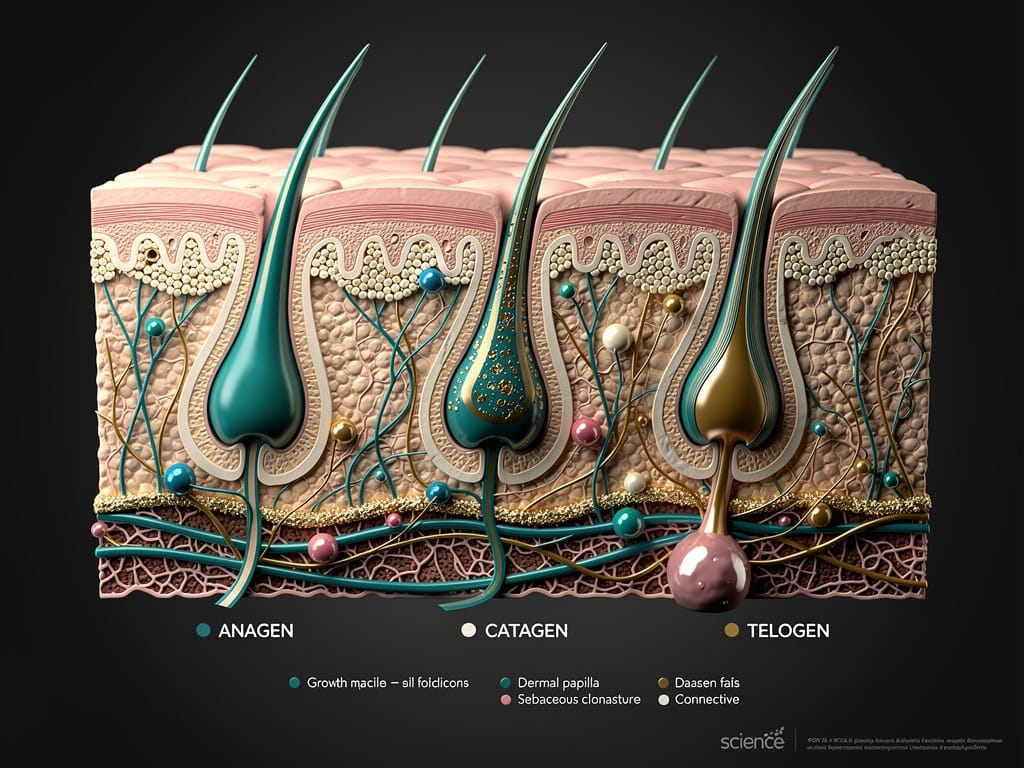
Estrogen is a biological anchor for your hair follicles. During high-estrogen phases - pregnancy, certain points in your cycle, or hormonal therapy - estrogen prolongs the anagen phase, which is the active growth stage of your hair cycle.
More follicles stay in growth mode. Longer. The hair feels thick, dense, almost electric.
Then estrogen drops.
The follicles that were artificially held in the anagen phase get a sudden biological signal to move on. They shift - all at once - into the telogen phase, which is the resting and shedding stage. This synchronized mass exit is called telogen effluvium.
Key Insight: The shedding you see is not damage happening now. It is the biological echo of a hormonal shift that occurred 8 to 12 weeks earlier. You are watching a delayed reaction.
This is why the timing feels so disorienting. The postpartum shed hits when you thought you were through the hard part. The menopause thinning appears years into the transition. The pattern is consistent, and once you understand it, it becomes something you can work with.
The Four Hormonal Transitions That Trigger This Response
Not all hormonal shifts are equal. But the estrogen withdrawal mechanism is the same across all of them.
- Postpartum: The most dramatic drop. Estrogen plummets within days of delivery. Mass telogen effluvium typically peaks between weeks 8 and 16 after birth.
- Perimenopause and Menopause: A slower, sustained decline. The shedding is less acute but more persistent. Follicle miniaturization - where hairs regrow progressively finer - becomes the primary concern here.
- Stopping Hormonal Birth Control: Synthetic progestins in certain pills suppress ovulation and alter estrogen signaling. Discontinuing them can trigger a withdrawal shed within 1 to 3 months.
- Post-Cycle Hormonal Dips: Even within a regular menstrual cycle, the sharp estrogen drop after ovulation and before menstruation can cause low-grade, recurring shedding in sensitive individuals.
The mechanism is the same. The intensity and duration differ.
Your Protection Blueprint - Step by Step

Here is the framework. This is not about reversing biology. It is about supporting the follicle environment so that the hairs that do regrow come back strong.
Step 1 - Stabilize the Scalp Environment First
A stressed scalp amplifies shedding. Chronic inflammation, product buildup, and poor circulation all compound the hormonal signal. Start with a weekly scalp exfoliation using a salicylic acid-based treatment to clear the follicular opening. Follow with a daily scalp massage - 4 minutes minimum - to drive blood flow to the dermal papilla, the structure that feeds each follicle.
Step 2 - Address the Nutritional Deficits That Hormonal Shifts Create
Estrogen fluctuation directly impacts how your body absorbs and uses key micronutrients. The ones that matter most for follicle function during a transition:
- Ferritin (stored iron): Low ferritin is the single most underdiagnosed driver of hormonal hair loss. Get a blood panel. Target levels above 70 ng/mL for hair health, not just the clinical minimum.
- Zinc: Supports the enzymes that regulate the hair growth cycle. Hormonal shifts deplete it faster.
- Biotin and B-complex vitamins: Support keratin infrastructure. Most people are not deficient, but absorption drops under hormonal stress.
- Vitamin D3: Directly activates hair follicle receptors. Deficiency is rampant and consistently linked to telogen effluvium.
Step 3 - Use Topical Actives That Speak the Follicle's Language
Two ingredients have the strongest evidence base for hormonal shedding specifically.
Minoxidil (2% for most, 5% for persistent cases): Extends the anagen phase and increases follicle size. It does not address the hormonal root cause, but it directly counteracts the biological mechanism of the shed. It works.
Caffeine-based topicals: Research from the International Journal of Dermatology shows caffeine penetrates the follicle and counteracts the suppressive effect of DHT - a hormone that rises in relative dominance as estrogen declines. Use a caffeine serum or shampoo with a 1 to 2 minute contact time.
Step 4 - Protect the Hair You Still Have
During active shedding, mechanical stress becomes a real threat. The follicles are already in a fragile transitional state. Simple rules:
- Switch to a wide-tooth comb on wet hair only. Never brush wet.
- Eliminate tight hairstyles. Traction on a transitioning follicle accelerates miniaturization.
- Drop the heat tools to below 350°F and use a thermal protectant every single time.
- Sleep on a silk or satin pillowcase. Friction matters more than people think.
Step 5 - Work With Your Doctor, Not Around Them
This is non-negotiable. A full hormonal panel - including estradiol, FSH, LH, thyroid function, and ferritin - gives you a precise picture of what is driving the shed. Some transitions warrant medical support: low-dose topical estrogen, hormone replacement therapy, or spironolactone for androgen-driven thinning.
Self-diagnosing and self-treating hormonal hair loss is like trying to fix a structural issue with paint. Get the data first.
Remember this: Telogen effluvium triggered by estrogen withdrawal is almost always temporary if the underlying hormonal environment stabilizes and the follicle is supported properly. The follicle is not dead. It is waiting.
The Bottom Line
Your hair is not betraying you. It is responding - with biological precision - to a shift in its hormonal environment. The shed is a signal, not a sentence.
Understand the mechanism. Address the scalp. Fill the nutritional gaps. Use evidence-based actives. Protect what is there. And get the clinical data to back your strategy.
That is how you stop reacting and start directing.